In a recent blog post I used driving a car as an analogy. Sometimes we arrive at our destination but can’t actually remember navigating that major junction. Our internal autopilot, based on a combination of familiarity, habitual decision making and muscle memory, has ensured that we get there safely. It’s an example of what is commonly referred to as ‘unconscious competence’. Many use this term to indicate the highest level in the development of comprehension or of a skill. But is this really the highest level? If we believe in the idea that we can always improve then this would suggest there must be something more. But what? Well, let’s go back to the beginning.
A simple model of progression
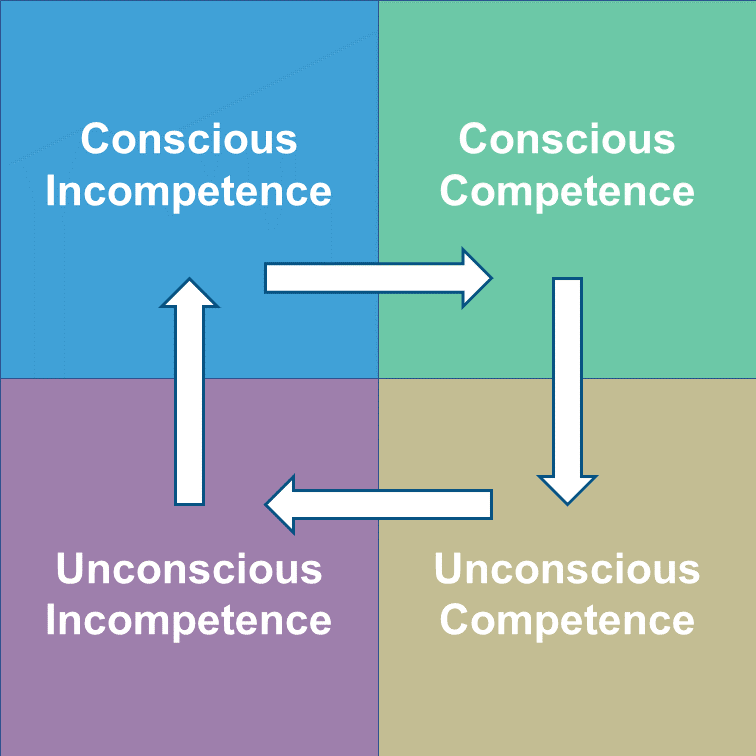
You may have encountered the conscious/competence model on our Teach the Teacher Course for Doctors or elsewhere in your training. Here’s a diagram to illustrate the four clear steps:

1: Unconscious-incompetence
This is where we don’t know what we don’t know. Ignorance is bliss – but unconscious-incompetents can pose a serious risk in many ways. When people are unaware of what could go wrong then disaster lurks just around the corner. Doctors working in teaching or leadership capacities who know the dangers are the ones who feel the pressure at this point. They are typically well versed in watching out for and managing such risks. We must choose the right time and right method to bring the issue to the learner’s attention, moving them to the next phase in a constructive manner.
2: Conscious-incompetence
Conscious-incompetence is often considered the most uncomfortable stage of the learner’s experience. Being aware that you don’t understand, can’t remember or are incapable of doing something that you want or need to do can be very stressful. Again, doctors who are teaching or leading others need to be aware of the multiple reactions to such stress and become skilled at guiding those in their charge to the next level.
3: Conscious-competence
This feels good for all concerned. It’s a safe and rewarding place to be. We get satisfaction from awareness of progress and confidence grows all round. But being conscious of absolutely everything that we are doing beyond the fleeting moment would be overwhelming. We need to concentrate and focus on the most demanding matters, so, as mentioned earlier, we have an internal autopilot which is designed to help us. It kicks in through repeated practise and experience as we progress to the in the fourth stage.
4: Unconscious-competence
Unconscious-competence would seem like the place to be – at the pinnacle of the pyramid. We can just get on with complicated matters with minimal effort. But what’s next?
What’s the next stage?
There have been numerous efforts to propose a fifth stage of development. Here’s the one that I find simplest and most useful which is based on a different diagrammatic representation of the model. To explain it, let’s return to the driving analogy.
On the day we sit our driving test we are definitely functioning in conscious-competence mode. We’re hyper-aware of everything we are doing. Once we get the good news that we’ve passed and gain our full licence we increasingly function in the unconscious-competence mode. We learn to listen to the music and chat to friends as we drive. The more familiar we become with the task, the more smoothly we drive and manoeuver the car. And what happens next?
Many of us start to go over the speed limit on a regular basis. We forget what some of those road-signs that we knew for the test mean. We start to function by expecting other drivers to do what we expect them to do. We’re less likely to notice that we cut across another driver as we change lanes. BANG!
The longer we spend in unconscious-competence the more likely we are to develop bad habits; to forget less commonly used facts and information; to fail to adopt and adapt new concepts into our practise. All too often, the next stage is actually a return to unconscious-incompetence.
An alternative?
An alternative approach is to regularly and deliberately return to conscious-competence. To revisit, remind, refresh and reset. This is one of the key reasons for ongoing CPD activity. The frequency of new discoveries and advancements in the technical aspects of a doctor’s knowledge far outstrips advancements in the social scientific matters: teaching; leadership; management; patient or team communication. Yet it is essential to regularly return to these topics to stimulate conscious-competence.
How effectively do you revisit, remind, refresh and reset yourself?
Stephen McGuire – Director of Development

 Doctors are members of one of the most ancient professions. Such membership brings the expectation of professional attitudes and behaviour. But what does it mean to be professional?
Doctors are members of one of the most ancient professions. Such membership brings the expectation of professional attitudes and behaviour. But what does it mean to be professional? We all take on many roles in our working lives. Our success is often dependent on an apparently straightforward but essential skill: giving quality feedback.
We all take on many roles in our working lives. Our success is often dependent on an apparently straightforward but essential skill: giving quality feedback. It’s now 10 years since the
It’s now 10 years since the  Do you want to change something? Well, start with ‘why’. People will follow you because they believe. So, if you can explain ‘why’ you want to change something and people believe your message then you’re more likely to get them on board. That’s the message shared by Simon Sinek in one of
Do you want to change something? Well, start with ‘why’. People will follow you because they believe. So, if you can explain ‘why’ you want to change something and people believe your message then you’re more likely to get them on board. That’s the message shared by Simon Sinek in one of  Cast your mind back 10 years to January 2009. How accurately would you have been able to predict the world as it is today?
Cast your mind back 10 years to January 2009. How accurately would you have been able to predict the world as it is today? Doctors hate their computers. Well, that’s according to Atul Gawande. The influential doctor and writer recently dedicated almost 9,000 words to outline his thoughts on the matter in The New Yorker’s
Doctors hate their computers. Well, that’s according to Atul Gawande. The influential doctor and writer recently dedicated almost 9,000 words to outline his thoughts on the matter in The New Yorker’s