 In recent years, some high profile writers, including Atul Gawande, (The Checkpoint Manifesto) and Matthew Syed, (Black Box Thinking) have drawn sharp contrast in the approach to learning from errors within healthcare when compared to aviation.
In recent years, some high profile writers, including Atul Gawande, (The Checkpoint Manifesto) and Matthew Syed, (Black Box Thinking) have drawn sharp contrast in the approach to learning from errors within healthcare when compared to aviation.
Aviation is, in relative terms, a young and technologically advanced industry. It is one where basic errors can result in catastrophe. The culture which has developed is one where there is belief that errors and malfunctions are inevitable in the face of complexity. Errors and malfunctions, from the minor to the disastrous, are opportunities to learn – not just for the individual, or the organisation, but for the industry as a whole.
Similar dramatic advancements can be witnessed in other arenas, including Formula 1 motor racing. The detailed, critical analysis in response to every incident means that we now regularly witness racing drivers walk uninjured from the most spectacular high-speed incidents.
The writers mentioned have presented the practise of medicine to be considerably different – with a culture which is problematic to learning and progress. They describe a culture where there is a lack of investigation, in awareness regarding the cause of errors, of avoidance and even concealment. Rather than suggesting any willful malpractice, one driver of this culture is identified as the historical, unhealthy, hierarchical reverence which results in a reluctance to challenge. Another driver is the well-meaning concern for the feelings of patients and relatives, to soften the blow when things have gone wrong. Doctors have learned to talk in euphemisms where ‘malfunctions’ and ‘mistakes’ morph into “complications”, or “unexpected outcomes” in a world where “I’m afraid these things happen”.
Aviation and Formula 1 have many advantages over medical practise. Financial investment of commercial organisations versus public services would seem like an obvious difference. Yet there is plenty of evidence to support the approach of reducing medical errors to reduce costs from further patient care and litigation. Aviation and Formula 1 do benefit from a variety of technical tools, including black-box recorders, a mind-boggling array of sensors and simulators.
While the tools themselves are difficult, if not impossible, for many medical disciplines to replicate, the underlying principles can be utilised:
- Reviewing the collated information enables the identification of any deviation from normality.
- Review is applied to minor as well as major incidents.
- Small errors are the early warning signs of future major incidents.
- The identification of patterns of errors should lead to change.
Thankfully, there are plenty of healthcare examples where significant progress has been achieved. One high-profile example is the Virginia Mason Health System in Washington which pioneered the Patient Safety Alert System. This review system, where healthcare workers report their own errors or safety concerns, is credited with transforming the hospital into a genuine learning organisation. As a result the Virginia Mason is now recognised as one of the safest hospitals in the world. However the change did not happen overnight. Doctors and other healthcare workers were initially reluctant to file reports and raise alerts as their attitudes were rooted in the previous culture. Eventually, they found that, other than in situations where they had obviously been reckless, they would be appreciated and not punished for presenting a problem. This in itself required a significant and sustained change in the leadership approach throughout the hospital: the acceptance that errors and malfunctions are inevitable in the face of complexity and are an opportunity to learn.
Of course, there are other high profile examples of similar progress. There are many examples where systems have been implemented in response to patterns of errors being identified. Where ideas have been shared, others have been able to build upon the successes – just as in aviation and Formula 1.
Problems, however, definitely still persist.
In 2015 the UK Government published a report into clinical incidents in the NHS. It concluded that processes for investigating incidents were in place but that the prevailing culture was preventing them from being effective. It found that the focus of reviews was ‘preoccupied with blame or avoiding financial accountability.’
To quote Matthew Syed: ‘This is the paradox of success: it is built upon failure.’ and from Dr Gary Kaplan of Virginia Mason: ‘We learn from our mistakes. It is as simple and as difficult as that.’
What are you doing to make the changes required in healthcare to make this learning a reality?
The challenges raised in the text and the solutions are explored in our new CPD accredited one-day course Practical Management for Doctors.
 The ideal patient-clinician relationship is one of concordance. A shared understanding is developed leading to the patient playing an active part in their care. They follow their agreed treatment plan to achieve the best outcome in the circumstances. If only we lived in an ideal world! Although there are many patients who diligently and effectively implement their plan there are many others who do not.
The ideal patient-clinician relationship is one of concordance. A shared understanding is developed leading to the patient playing an active part in their care. They follow their agreed treatment plan to achieve the best outcome in the circumstances. If only we lived in an ideal world! Although there are many patients who diligently and effectively implement their plan there are many others who do not.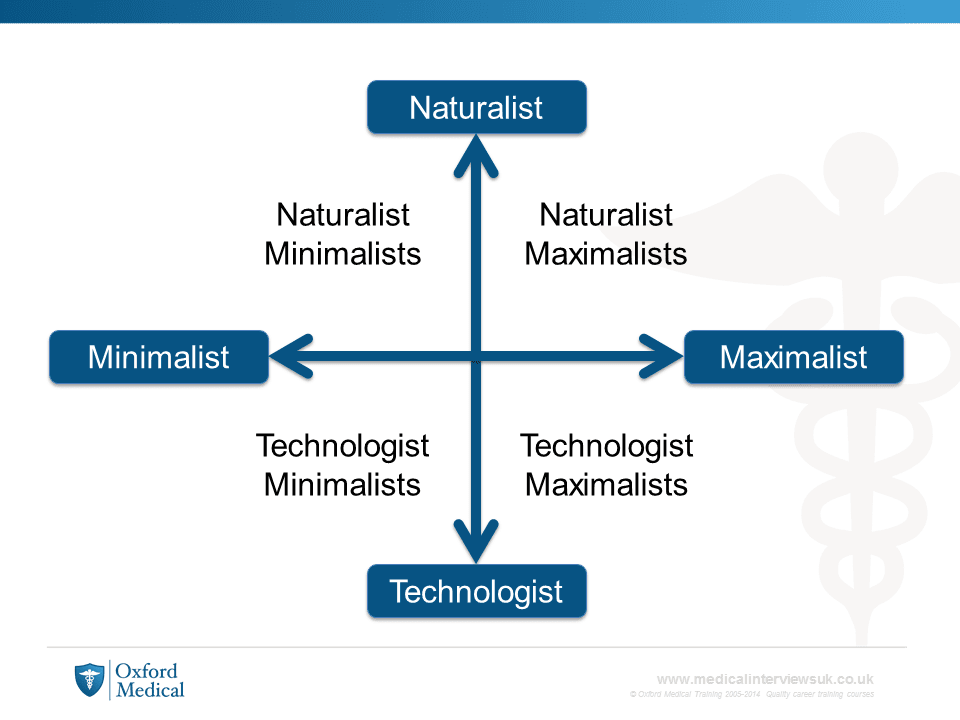

 Since our launch in 2004 we have grown our list of regular course locations to include London, Oxford, Nottingham, Leeds/Wakefield, Manchester and Glasgow. We also offer a growing selection of
Since our launch in 2004 we have grown our list of regular course locations to include London, Oxford, Nottingham, Leeds/Wakefield, Manchester and Glasgow. We also offer a growing selection of  Any preventable death is a tragedy. The impacts are wide and varied. Families, carers, doctors, nurses and wider healthcare teams can all be affected. Though it is impossible to turn the clock back it is essential that one response to any such event is a thorough and robust review. Since the failings at Southern Health Foundation Trust he CQC has been exploring the processes of review and investigation of patient deaths in the NHS. The output is the publication of a report titled
Any preventable death is a tragedy. The impacts are wide and varied. Families, carers, doctors, nurses and wider healthcare teams can all be affected. Though it is impossible to turn the clock back it is essential that one response to any such event is a thorough and robust review. Since the failings at Southern Health Foundation Trust he CQC has been exploring the processes of review and investigation of patient deaths in the NHS. The output is the publication of a report titled  A key point in Report of the Mid Staffordshire NHS Foundation Trust Public Enquiry from 2012 was a call for ‘the recognition that healthcare management and leadership is, or should be treated as a profession‘.
A key point in Report of the Mid Staffordshire NHS Foundation Trust Public Enquiry from 2012 was a call for ‘the recognition that healthcare management and leadership is, or should be treated as a profession‘.
 The course described two frameworks for understanding what makes a successful team: the Healthy Teams model, which outlines the key requirements of a team, and the Five Dysfunctions of a Team, which illustrates elements which may cause problems within a team and thereby result in ineffective teamwork and poor results. I found that these frameworks were useful ways to think about working in a team, and although a lot of the material covered was information I had either been told previously or had thought about in abstract, I found it much more practical and memorable to aggregate the various concepts into more formal structures. The components of the Healthy Teams model and the Five Dysfunctions of a Team were each described in detail, as well as ways in which each requirement of a healthy team could be affected by the relevant dysfunction. While working through the course, I was able to put the concepts described into the context of my own experiences when teams had worked well (and not so well), and the questionnaire at the end helped me to reflect on how my individual performance might have contributed to these outcomes. I found the sections on common goals and effective feedback particularly relevant, as forming goals and giving and receiving feedback are areas that I have had difficulty with in the past.
The course described two frameworks for understanding what makes a successful team: the Healthy Teams model, which outlines the key requirements of a team, and the Five Dysfunctions of a Team, which illustrates elements which may cause problems within a team and thereby result in ineffective teamwork and poor results. I found that these frameworks were useful ways to think about working in a team, and although a lot of the material covered was information I had either been told previously or had thought about in abstract, I found it much more practical and memorable to aggregate the various concepts into more formal structures. The components of the Healthy Teams model and the Five Dysfunctions of a Team were each described in detail, as well as ways in which each requirement of a healthy team could be affected by the relevant dysfunction. While working through the course, I was able to put the concepts described into the context of my own experiences when teams had worked well (and not so well), and the questionnaire at the end helped me to reflect on how my individual performance might have contributed to these outcomes. I found the sections on common goals and effective feedback particularly relevant, as forming goals and giving and receiving feedback are areas that I have had difficulty with in the past. An open letter to the BMJ.
An open letter to the BMJ.