Each year, we expect the seasons to follow a very familiar pattern. However, the career progression calendar for doctors is always far more predictable than the weather. In early August, a new cohort arrives fresh from medical school. At the same time, those in their Foundation Years progress to their new level and their latest rotations. As they do so, plans for next year come into focus.
For many, this includes wanting to secure a place on a training programmes such as IMT, ACCS or CST. Though the exact dates for application windows opening and deadlines may not always be known as far in advance as we’d like, they’re still more predictable than the weather!
To help, we’ve created a dedicated webpage which provides you with an overview of the recruitment process. We include explanations of the self-assessment and interview stages. In addition, we also include essential advice on how to best prepare yourself for success.
Completing your application for a training post can be a challenging task. You want to ensure that you stand out from the crowd by presenting the full breadth and depth of the experience that you’ve gained to date. At the simplest level, this means submitting the strongest application you can. For example, you will want to score as many points as possible on the self-assessment for IMT, or to achieve the highest grade indicator when your are uploading your index page for CST. However, it’s essential that you are honest when claiming your points or indicators and follow the guidance correctly.
On this webpage, we provide you with some background, an overview of how our various Teach the Teacher Courses relate to different recruitment processes, followed by a detailed look at each of the most popular programmes and, finally, other points to consider.
Every year, large numbers of doctors contact us with questions about using our courses to support their application. Many are confused about the points and indicators they can claim for the various “Teach the Teacher” course formats that we offer. It essential to be aware that different programmes use different scoring systems and that the criteria has changed over time. Sometimes, the criteria has changed at very short notice, just before the application window opens. Considering the high competition rates, it’s understandable that some doctors can become quite anxious about making the right choices.
In autumn 2024, after another very late and fundamental change to one major programme’s scoring criteria, we brought the issue to the attention of the BMA Resident Doctors Committee and explained the impacts. How can any doctor make proactive, informed choices about their development when the requirements can unexpectedly change at the last minute? The Committee, in turn, took this matter up with the decision makers.
Although we take every effort to ensure that information we provide is up to date, we encourage you to make your own checks and to see full details. Links to sources of information are provided throughout this page.
The good news is that we believe last minute changes to scoring criteria should be a thing of the past.
Summary table of Teach the Teacher courses and training programmes
If you’ve already taken a course, then you will want to ensure you claim the correct number of points or choose the correct indicator. Alternatively, if you are still considering which course to take, then you want to ensure your make the best choice.
So, which course and what score or indicator?
Here’s a table to summarise the latest publicised scoring for the biggest training programmes and our most popular Medical Teaching Course options.
*Further appoints available within relevant domains for both Ophthalmology and Histopathology.
For clarity, the following sections outline the differences between the training programmes to help you further.
IMT, ACCS and other Physician Higher Specialty Training programmes
The self-assessment scoring for these programmes are all aligned. Here is a copy of the summary table in the “Training in Teaching” domain on the IMT Recruitment Application scoring webpages.
For IMT/ ACCS and others Physician Higher Specialty Training: Option
Score available
Notes
I have a higher qualification in teaching e.g. PG Cert or PG Diploma.
3
This could be full time over one academic year or part-time over multiple years.
I have had training in teaching methods which is below the level of a PG Cert or PG Diploma
1
This should be additional to any training received as part of your primary medical qualification. Training should be delivered with a duration of at least six hours (i.e. a one-day course) of synchronous (live) teaching time.
I have had no training in teaching methods.
0
For applications at CT1 level to IMT, ACCS and the list of programmes coordinated by the Physician Specialty Recruitment Office (PSRO) , you score 1 point for our tutor-led 2-day Teach the Teacher Course for Doctors , whether you take the course in our Virtual Classroom, or in-person. Both formats fulfil the criteria of “synchronously delivered teaching” and being “taught by a live teacher”. Our 3-day Extended Teach the Teacher Course will provide you with a broader experience but the same scoring for these applications.
Our instant-access Teach the Teacher Online Course is designed for you to work through alone and at your own pace. It does not involve a live tutor, and therefore cannot currently be used for IMT or ACCS self-assessment scoring.
Candidates will no longer be asked to complete self-assessment on Oriel.
Instead, candidates invited to interview will be requested to upload an index page with the appropriate indicators for each domain.
Candidates will assign a letter from A to E to each domain showing which category of evidence they think their evidence sits in (A being the top, E being the bottom).
The portfolio has moved to this structure as the category acts as a guide for the assessor and is not the final score allocated – this is determined during the interview.
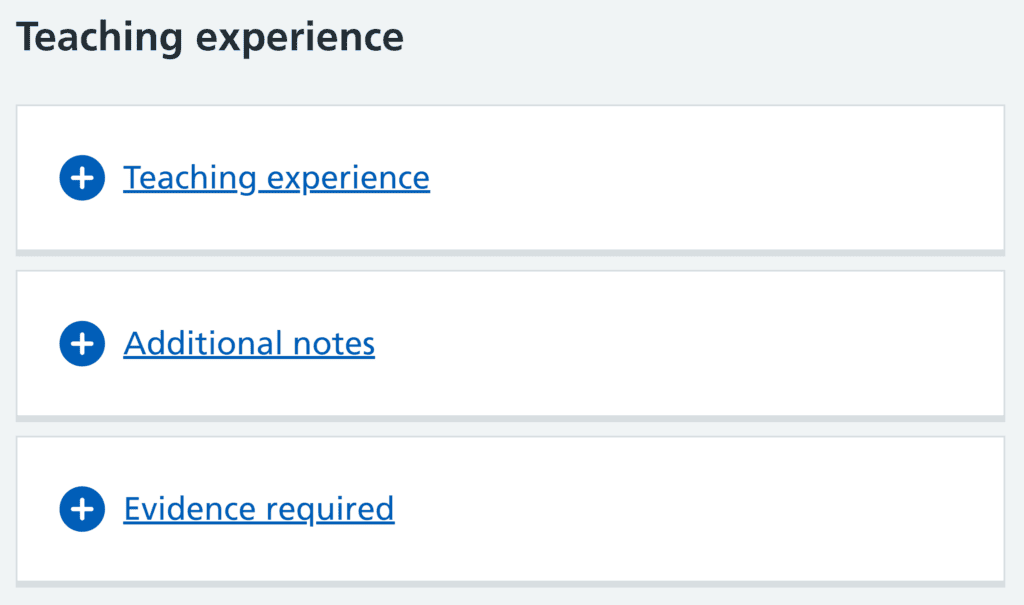
Although the previously listed “Training Qualifications” domain was removed from the process, Teach the Teacher Courses are still relevant for CST recruitment within the “Teaching Experience” domain.
Here’s a screenshot from the “Commitment to specialty (all surgical specialties)” indicator guidance section near the bottom of the NHS webpage.
Expanding the “Training experience” tab describes the indicator to select when uploading your index page. It includes the following information as the last two entries on the table.
For CST1: Teaching Experience Options
Indicator
Notes
. . . Or I have undertaken some educational activity focused on learning to teach
D
This would include any form of educational event focused on learning the skills of teaching – such as a training the trainers course online or otherwise
I have not provided teaching
E
Information under the Evidence required” tab states:
“A certificate for the educational event focused on learning how to teach”
So, the certificate which you receive for completing any of our Teach the Teacher courses means you can select indicator D on the scale of A-E.
It’s important to note that your final grade for Teaching Experience will be determined by your assessor during interview. So, being able to confidently explain what you learned from your course and how you have used the skills and knowledge gaining will be essential for your success.
For CST1 programme applications, you can select indicator D for any of our Teach the Teacher courses, including 2-day tutor-led Teach the Teacher Course for Doctors, whether that is taken in our Virtual Classroom or In-person, our 3-day Extended Teach the Teacher Course, or our Teach the Teacher Online Course where you gain access to materials which you work through on your own or at your own pace.
Hold a formal teaching qualification awarded at postgraduate level, for example: masters, CILT, PGDip, PG Cert
A
Have made a major contribution to a national or international teaching programme, with evidence
B
Evidence of other training in teaching methods after study of at least 2 days (such as Train the Trainers)
C
Have evidence of providing regional teaching
D
None of the above
E
For Clinical Radiology ST1, you score category C for our tutor-led 2-day Teach the Teacher Course for Doctors, whether you taken in our Virtual Classroom, or in-person. Our 3-day Extended Teach the Teacher Course will provide you with a broader experience but the same scoring for Radiology applications.
Our instant-access Teach the Teacher Online Course is designed for you to work through alone and at your own pace. It does not involve a live tutor, and therefore cannot currently be used for Radiology ST1 applications.
Ophthalmology ST1, Education & Teaching
The Ophthalmology ST1 Evidence Folder for recruitment takes a different approach from other specialties in that it utilises cumulative scoring within domains. Here is a summary of the Education & Teaching domain from the Evidence Folder guidance.
CUMULATIVE SCORING (max score 5pts)
Ophthalmology ST1
0.5 points each
– for helping with an educational course (more than one session), designing an e-learning tool, writing an e-book, completing a “teaching the teachers” course and/or undertaking a formal role in examining undergraduates.
1 point
– for contributing to at least three teaching sessions on different subject areas over a period of at least 3 months with formal feedback uploaded.
2 points
– for a Higher teaching qualification e.g. a Diploma, Certificate in Medical education.
2 points
– for writing a chapter in a postgraduate-level academic book.
3 points
– for writing a postgraduate-level academic book.
Cumulative scoring for Opththalmology means that you can be recognised for 0.5 point for taking any of our Teach the Teacher courses PLUS additional points for any of the other criteria listed.
For Ophtalmology ST1 applications, you score 0.5 points for any of our Teach the Teacher courses, including 2-day tutor-led Teach the Teacher Course for Doctors, whether that is taken in our Virtual Classroom or In-person, our 3-day Extended Teach the Teacher Course, or our Teach the Teacher Online Course where you gain access to materials which you work through on your own or at your own pace.
I have had substantial training in teaching methods lasting more than 2 days; this could include a completed module which forms part of a postgraduate teaching qualification
2
I have had brief training in teaching methods lasting no more than 2 days
1
I have had no training in teaching methods
0
For Histopathology ST1 applications, you score 1 for any of our Teach the Teacher courses, including 2-day tutor-led Teach the Teacher Course for Doctors, whether that is taken in our Virtual Classroom or In-person, or our Teach the Teacher Online Course where you gain access to materials which you work through on your own or at your own pace.
Completing the application is only the first hurdle in achieving your training post. If you are successful in getting through to interview then you have the challenge of presenting yourself at your best during the intensive interview process. So, you need to gain as much experience in numerous areas between now and then. You will need to demonstrate your patient communication, team communication and leadership skills. Taking courses in these subjects will give you fresh input and help you to clarify your thinking. Being able to show that you have put ideas gained from course theory will always improve your chances of success.
And it’s always worth considering a dedicated interview preparation course to help you pull everything together.
In this video interview, Dr Chris Boyson, Director of GMC Appraisals.com, outlines the relationship between CPD and appraisals for doctors. He explains the CPD requirements for maintaining GMC registration and draws attention to the importance of professional skills development, such as communication, reflective practice, teaching, leadership and management. Chris also describes how development of professional skills can improve a doctor’s employability and the particular relevance this has for International Medical Graduates, (IMG’s).
About GMC Appraisals.com
GMC Appraisals.com provide affordable high quality medical appraisals for both UK and international doctors. Doctors who utilise GMC Appraisals.com services are entitled to a 10% discount on any Oxford Medical courses*.
What are your thoughts and feelings about annual assessments and reviews? ARCP’s? Appraisals? CQC inspections? Audits? Or any of the many other process where you or your team come under periodic scrutiny?
At Oxford Medical, we’ve recently completed the annual assessment required to retain our Customer Service Excellence hallmark from the UK Government Cabinet Office. In keeping with many other regular review processes, this required us to collate information, create reports, submit documentation and participate in long discussion meetings. It’s not like we didn’t have other stuff to be getting on with. We had to respond to searching questions, listen to feedback and then digest a detailed report.
There’s no legal requirement for us to retain this hallmark. We do this by choice. So, you may be wondering . . .
Why would you put yourself through this?
If your Annual Appraisal or ARCP was voluntary, would you take part? Would you prefer to skip all those those audits, reviews and inspections? Imagine what you could do with the time you’d gain without all the associated admin. Imagine avoiding all that last minute rush and the discomfort that comes with having to explain your actions, inactions and responses to events. But life’s not like that.
The easy way isn’t always the right way and, assuming you want to stay registered and make progress, participation in these governance processes is a fact of your professional life. Without doubt, for all their good intentions, the systems and those who run them are far from perfect. For the vast majority of us, making any fundamental change to the way they are implemented is beyond our control. However, the choices we make, the attitude we take and the way we partake can make the fundamental difference between this being time that is well spent, or wasted.
Our attitudes are closely tied to our beliefs, and our beliefs, including our perception of our abilities, are shaped by our experiences.
So, what do you believe?
Is it safe to assume that you believe there is value in pausing to reflect on your experiences and to learn from them?
There’s much to be gained by being open and honest with ourselves about our short-comings. Why did this go wrong? Where are the gaps in my abilities? Where might I have regressed? What are the impacts? Why does it matter and what can I do about this?
Equally, we can all gain a real boost from standing back to see the progress we’ve made. What’s changed for the better since the last time? How did you achieve that and what’s the impact? How can you make good use of that going forward?
Developing your abilities to make progress
When it comes down to it, all of these review processes are intended to maintain and improve standards. The output should be improved awareness, decisions to take constructive action and continue progressive development.
Unfortunately, there’s one skillset that is fundamental to all of these processes which is neglected all too often: the skills related to reflective practice.
Reflective practice is a very personal matter. What works for your friends or colleagues will not necessarily work for you. Investing time to develop your personal approach to reflective practice can make a huge difference. Regular reflection with effective methods can significantly improve efficiency of preparation for ARCP, appraisal or any other review. It can shift the balance from ineffective tick-box to high impact engagement, where you participate for personal benefit.
Our annual Customer Service Excellence assessment has enabled us to recognise and celebrate our progress, identify areas for improvement and to define actions to achieve this. We look forward to repeating the process next year and have already taken steps to make it easier to collate our information as we go.
What steps are you taking to get the most out of these governance processes?
Following the recent launch of our Reflective Practice for Doctors Online Course, we’ve refreshed our range of Online Career Development Collections. We’ve curated selections of our instant access online courses into packs. Choosing the right pack to match your personal needs both broadens your learning experience and saves you money.
Here’s a summary of the key changes.
We’ve expanded our two flagship packs to include the new course:
There’s an expectation that all doctors participate in reflective practice – but the majority are not taught how to do this well.
Learn to reflect for your own benefit, converting your thoughts into action or into written submissions.
After listening to the needs and interests of doctors attending our courses, we’re delighted to introduce the latest addition to our range: Reflective Practice for Doctors Online Course.
It’s accredited for 4 CPD points:
Learn to reflect for your own benefit, converting your thoughts into actions or into written submissions.
Have you ever wanted to learn ballet in the company of other doctors? What about origami then? Counting to ten in Japanese? How to draw cartoon characters? Would you like to learn how to play Chinese Poker? A card trick that could baffle your friends? How to strike the perfect yoga tree pose? Or would you like to learn how to juggle?
You might be thinking, “Ah, it’s 1st April today!” True. Yet all of this and more can happen on our two day Teach the Teacher Course for Doctors.
For a short time on this course, we step away from the medical world and explore other subjects. Anything goes. And you will find yourself teaching something that you know about. This gives you the opportunity to practise teaching something and experience other people teaching something. Yes, it can be a lot of fun. But more than that, it frees you and your fellow delegates to experiment. We then consider how the various styles and approaches of teaching can be brought back into your role as a doctor.
It’s a great way to improve your teaching. No previous ballet experience required!
Update 2025: Our original post is from back in 2019. Although we now run the vast majority of our course online via our Virtual Classroom, we still use our approach of stepping away from the medical world to help explore learning teaching. We can’t predict which subject your fellow delegates will decide to teach when you attend. But, we can guarantee that we will always make it relevant to your teaching practice as a doctor.
Have you ever seen a model ship in a bottle? How do they do that? It obviously doesn’t fit through the bottleneck. So, how do they get it in there?
Like most things, creating the ship in a bottle requires the right knowledge, skills and attitude. First of all, you need the knowledge of the process and how to pull it off. Second, you must acquire a set of skills ranging from designing the model through to having a very steady hand and using tools in confined spaces. Success also depends on having the right attitude, including a great patience and perseverance for when you slip unexpectedly or get stuck in the wrong place.
What’s that got to do with resident doctors?
In a recent interview, Philip Banfield, the BMA’s chair of council, discussed the “mess” of the current UK training system which “bears no relationship to the workforce needs.” He illustrated this with the example of training in anaesthetics. Last year there were several thousand applicants for just a few hundred training posts at a time when the UK has a shortfall of around 1,900 qualified anaesthetists.
There was an average of 4.7 applications for each available post
For Emergency Medicine (ACCS) CT1/ST1 the competition ratio was 7.6
For CT1 Core Psychiatry Training it was 9.5
Clinical Radiology ST1, 11.9
Ophthalmology ST1 had 14.4 applicants per post
Public Health Medicine ST1, 17.5
Neurosurgery ST1 was 19.7
And what about competition for Cardiothoracic surgery ST1? There were over 45 applicants for each available post.
Now consider these figures in conjunction with the well documented shortage of qualified consultant grade doctors, with the direct impact this is having on waiting lists and locum costs. It’s very clear there’s a restrictive bottleneck in the training and workforce planning system.
Any job selection process is effectively a competition. Unfortunately, the data can make the process of applying for and securing a training post seem more like a lottery.
So, how do you give yourself the best chance of winning?
Well, to win a lottery, you need to buy a ticket. The more tickets you buy the better chance you have of winning. That logic may well be one of the factors that is impacting the data. It would appear that numerous doctors making multiple applications is inflating the competition rates for some programmes. That may well be true, but the bottleneck still exists.
So, how can you give yourself the best chance of squeezing through the bottleneck and onto the training programme of your choice?
Let’s go back to getting the ship in the bottle.
You give you best chance by focusing on acquiring the right knowledge, skills and attitude.
Yes, you need acquire the appropriate base level medical knowledge, but bear in mind that it’s highly likely that every other applicant will have that too. So you need a bit more. You need to have knowledge of the system. For example, what are the scoring criteria for being shortlisting candidates for the training programme you are interested in? We provide links to reliable sources of information in our various blog posts and free information.
Once you know what’s required, then you can set about gaining the appropriate skills and experience. Again, this is more than direct medical or surgical skills. Dependent on the programme you are applying for, you are likely to improve your chances through evidence of participation in audit, contributions to publications and for training and experience in teaching. When it comes to the interview stations, you may well need to excel in a patient communication scenario or delivering a presentation.
Next, let’s think about attitude.
You will improve your chances if you are proactive and do the right things for the right reasons. Don’t wait to be asked if you want to participate in an audit or in developing a poster or research paper. Make enquiries in your current post about how you can contribute. Don’t just take courses to get points to tick a box. Take useful courses that will genuinely support your development. And don’t wait to take courses at the last minute. Take your Teach the Teacher,leadership or communication skills course sooner rather than later. That way, you have the opportunity to put what you learn into action and gain genuine experience. You will then be well placed to share those experiences, to demonstrate you knowledge and abilities when it comes to the interview stages.
If you’re involved in supporting resident doctors who are aspiring to securing a training post, then you will do well to encourage them in this direction.
And if you are one of those resident doctors, what steps are you taking to give yourself the best chance of squeezing through the training bottleneck?
By Professor Dr Jacqueline Baxter. Professor of Public sector leadership and management.
Jacqueline Baxter is professor of Public Leadership and Management at The Open University UK and a longstanding member of Oxford Medical’s Faculty of Tutors. Her research interests lie in the areas of leadership emergence, leadership strategy and identity, plus online teaching and learning. You can find her on LinkedIn at: https://www.linkedin.com/in/professor-jacqueline-baxter-53206a12/
Remote meetings are, in my experience, often poorly chaired, lack structure and value and take up employees valuable time. Since the pandemic, meetings often run back-to-back, meaning people arrive in them unprepared and still thinking about the last meeting. In addition, meetings have increased as the time it takes to get from one to another has now been eradicated, along with the thinking and down time this used to provide. A good question to begin with is why are we having this meeting and what do we hope we are going to achieve ? Not all meetings are necessary. Some meetings can be avoided by other means of discussion – Padlets that illustrate others’ thoughts in a productive way, online polls etc.
But if you do have to have a meeting, just like any other type of remote interaction, remote meetings take thought and preparation. Some of the ways that you can make your meetings better are outlined below:
Setting a clear agenda and stating why this meeting is necessary
People often do the former and forget the latter! Have you made it clear why people should be attending your meeting? I have often been in meetings where I have felt completely redundant. Either because the topic was out of my scope of interest, or because no one actually asked my opinion throughout the whole 2 hours! Or stated why it might be relevant.
A clearly defined agenda is fundamental to the success of remote meetings. Chairs should communicate the purpose, goals, and structure of the meeting in advance, ensuring participants understand their roles and what is expected of them (Mroz et al., 2018). Providing a detailed agenda enables attendees to prepare effectively and fosters a sense of accountability. Define who is accountable for what, preferably before the meeting. Which brings us to …
Getting people psychologically into the room!
Yes they are there, their cameras are on and their faces are on screen, but are they there? Compacted schedules due to increased online meetings are common now, across the public services. Leaders report back-to-back meetings from 8 am until 6pm, leaving precious little time for anything else. If you are dealing with back-to-back meetings, chances are that you will still be thinking about the last one, when you come into this one…
How can you, as chair, set a question before the meeting, that gets people into the room? Or create a short mindfulness exercise to give people the space to reflect on the subject of their current meeting.
Establishing your ground rules
Setting clear ground rules regarding punctuality, muting microphones, and minimizing multitasking can help maintain focus. Research by Rogelberg et al. (2006) highlights the importance of meeting norms in enhancing group cohesion and productivity. For example, if you want to see people interacting ask for cameras on when they are a) either asked a question or b) respond to a question. Using the chat box can be handy if you want to get a response from everyone, but take care, you need to outline that this is what chat is for. If you are using breakouts for a meeting, make sure everyone is familiar with what happens when you put people into a group – if they are not, they may suspect a tech malfunction and leave!
Utilising tech effectively
Leveraging appropriate tools and platforms is critical for remote meetings. The chair should ensure that the chosen technology supports the meeting’s objectives, whether it involves video conferencing, shared documents, or interactive polls. According to Dennis et al. (2008), the alignment of meeting tools with the task at hand improves efficiency and participant satisfaction. Polls, quizzes and other apps can enhance collaboration (Baxter, 2024) and encourage quieter members of the group to voice opinions in a safe space. Which leads us to…
Encouraging inclusivity and participation
Remote meetings can amplify the challenges of unequal participation; for example, introverts can ‘disappear’ in larger meetings. Chairs can actively encourage all attendees to contribute by directing questions to quieter participants and acknowledging their input. They can also use names (much easier in the remote environment), enhancing psychological buy in (Cutler et al., 2021). This approach aligns with the findings of Pentland (2012), who demonstrated that inclusive communication patterns lead to more effective collaboration.
Preparing people in advance helps with engagement. If they haven’t had time to read the papers, give them time in the break and don’t be afraid to juggle the agenda items accordingly. Remember the meeting needs to be worth your time and others, so do what you have to make it so !
Managing time effectively
I become really worried if I don’t know when my breaks will be in a meeting. I also become tired, frustrated and start looking through my emails if the chair doesn’t outline when the break/s will be.
Time management is particularly crucial in remote settings where attention spans can wane. There is plenty of evidence that indicates that attention spans in remote environments are short. Allocating time for each agenda item, monitoring adherence to the schedule, and ensuring discussions remain focused are all parts of a remote chair’s job. Paying attention to people who have switched off cameras or are clearly scrolling the internet, is also part of the mix. Of course you can’t force people to engage, but you can create an environment where it becomes more likely that they will.
Effective time management not only increases productivity but also respects participants’ time constraints (Leach et al., 2009). Plentiful comfort breaks that are outlined from the start, can help with individuals’ management of meetings and colour their expectations and experiences. If a meeting looks likely to go on outside the given time, ensure that you alert people to this at the earliest opportunity, ideally at least 15 mins before the originally scheduled end point. This helps you reach agreement on whether to either extend the meeting, or carry points forward to another time. There is little worse than people ‘dropping off’ a call, leaving you sitting alone in the room…
Monitoring engagement online
Non-verbal cues are harder to read in remote meetings, making it essential for chairs to monitor engagement through active questioning and periodic check-ins. Research by Allen et al. (2015) suggests that maintaining engagement requires a combination of verbal interaction and visual aids, such as slides or screen-sharing. However, bear in mind that slides take up screen space – if people are joining by phone or tablet this will limit interaction. Polls do a good job of monitoring interactions, by providing a visual representation of people’s thoughts. The humble chat box can also be used for this, although you should make clear what you want the chat box to be used for at the beginning of the meeting. I have been in meetings where individuals were criticising the chair, in the chat box!
Providing summaries and action items
As with any meeting, the chair should conclude the meeting with a summary of key points and clearly defined action items. This practice ensures accountability and aligns with the recommendations of Cutler et al, (2021), who emphasise the role of follow-ups in sustaining meeting effectiveness.
Fostering a positive atmosphere
Finally, a positive and supportive tone set by the chair can influence the overall meeting atmosphere. Encouragement, humour, and expressions of gratitude contribute to a collaborative and motivated group dynamic (Fredrickson, 2001).
Conclusion
The chair’s role in remote meetings extends beyond mere facilitation; it involves creating an environment that fosters collaboration, inclusivity, and productivity. By setting clear agendas, utilising technology effectively, and ensuring participation, chairs can add significant value to remote meetings, benefiting both the attendees and the organisation as a whole.
References
Cutler, R., Hosseinkashi, Y., Pool, J., Filipi, S., Aichner, R., Tu, Y., & Gehrke, J. (2021). Meeting effectiveness and inclusiveness in remote collaboration. Proceedings of the ACM on Human-Computer Interaction, 5(CSCW1), 1-29. \
Dennis, A. R., Fuller, R. M., & Valacich, J. S. (2008). Media, tasks, and communication processes: A theory of media synchronicity. MIS Quarterly, 32(3), 575-600.
Fredrickson, B. L. (2001). The role of positive emotions in positive psychology: The broaden-and-build theory of positive emotions. American Psychologist, 56(3), 218.
Leach, D. J., Rogelberg, S. G., Warr, P. B., & Burnfield, J. L. (2009). Perceived meeting effectiveness: The role of design characteristics. Journal of Business and Psychology, 24(1), 65-76.
Mroz, J. E., Allen, J. A., Verhoeven, D. C., & Shuffler, M. L. (2018). Do we really need another meeting? The science of workplace meetings. Current Directions in Psychological Science, 27(6), 484-491.
Pentland, A. (2012). The new science of building great teams. Harvard Business Review, 90(4), 60-70.
Season’s greetings from all at Oxford Medical Training!
Over the festive period, you can make purchases, book spaces on courses and access your online courses via our website as normal. If you need to contact us for any reason, here is a list of our office hours over the 2 week holiday period, (all times GMT):
You can book courses, purchase materials, and access your online courses through our website as normal during this time.
If you contact us by email ([email protected]), then we will receive your message and respond when we return.
Should you have any urgent queries before that time, then please call 0131 526 3700 and leave a message. We operate a monitored out-of-hours answerphone service and will respond as appropriate.
Our Frequently Asked Questions page provides answers to the majority of queries we receive and may quickly provide you with the information you need.
Have a peaceful and happy festive period and we look forward to a fantastic 2025.